Today is my 66th birthday, so I am hoping that you will forgive an article that is at core the anecdotal ramblings of an old man.
It was inspired by horror at Wes Streeting (I could end the sentence there but I shall continue it) ‘s plan to give weight loss jabs to the unemployed.
The unemployed are more likely to be underweight than the population average, and this attempt to portray the unemployed as lazy couch potatoes is vile in many ways. Its masking as an “investment” in the economy by Big Pharma is chilling.
If it goes ahead, how many years do you think we are away from those who refuse to have the drug injected into their veins, having their benefits stopped?
How are we to view this attempt to use the “unproductive” as lab rats for Big Pharma?
It has also been announced that the government is to send employment advisers into mental health wards to try to get sick people back into work. This is astonishing. It is extremely difficult to access any mental health care at all on the NHS.
To get residential care requires in truth a level of mental health crisis that indicates a threat to life of yourself or others. Yet people from mental health wards are going to be got into work, when there are hundreds of thousands of perfectly well people desperate for a good job who cannot find one?
What is the purpose of this nonsense other than propaganda and stigmatisation of the unemployed?
Which leads me to my anecdotes on the NHS and its purpose.
Sixty years ago or so, when my siblings or I were sick enough to be in bed, my mother would phone the surgery and the GP would come to our home to see us. This was perfectly normal. It is probably difficult for Generation Z to believe this really used to happen.
Now if I am sick enough to be in bed, I have to phone the surgery precisely at 8am and go through the lottery of getting in to the phone queue, rather than the engaged signal as the queue is at capacity. I may have to call numerous times.
If I do manage to get into the queue I have to hope I get to the front of it before all appointments are taken. If I fail, I cannot make an appointment for the next day but have to try my luck again then, once more at precisely 8am, while a hundred other people are trying exactly the same thing.
If I am fortunate enough to make it through the queue, I am de facto triaged by a receptionist with no medical qualifications but to whom I have to explain my medical symptoms.
She will then, if she thinks I have a case, explain my symptoms to a doctor and I may come out of this process, not with the doctor coming to my home, nor with me attending the surgery, but with a phone call from the doctor and a down the line diagnosis.
I find that everybody I have spoken to – and from all parts of the UK – has to put up with the same system. I cannot believe we have fallen in to accepting this.
It is not medical treatment. It is not a national health service, it is a notional health service.
If I feel really bad I can attempt to bypass the system and go to the hospital Accident & Emergency service, which I will find clogged with scores of other desperate people, waiting hours and hours to try to get medical attention.
I have not told this story before, but about three years ago I was invited to a party in Ealing after one of the Assange hearings. I had just one glass of wine and started to feel dizzy and nauseous, so I made my excuses and left.
I got a taxi back to the hotel near the Old Bailey where I was staying, but collapsed in the street just across from the hotel. I vomited and could not stand up. The problem was my heart condition. I phoned 999 and was told by the ambulance service it would be approximately three hours before an ambulance could reach me.
Passers by assumed I was a drunk or drug addict and gave me a wide berth. After a very cold half hour (it was I think February) a group of Irishmen stopped to help me and carried me into my hotel. I quite soon fell asleep on the bed and the next morning felt fine – and went back into court.
I spent several months this year living in Greece. I had very bad bronchitis and pitched up at the local rural medical centre, the equivalent of the GP surgery. I was seen immediately by two doctors, examined at length, X-rayed and given an ECG and left with prescriptions, all within an hour of turning up.
Some months later I fell and dislocated my shoulder, in a highly remote rural location and after midnight. An ambulance arrived within half an hour and drove me for 90 minutes to the hospital in Volos, where my shoulder was reset.
Now here is the kicker. UK spending per capita on public healthcare is twice Greek spending per capita on public healthcare.
Yet while we spend twice as much, the experience of this patient (I did warn you this is going to be personal and anecdotal) is that key aspects of the Greek system are far better.
The NHS is in a state of near disaster. The reason is that it has been hollowed out for private profit, with the designated “profit centres” which give a high return hived off to private contractors (though not visibly to the patient), and the public purse left paying for the complicated and expensive bits.
Of course, we hear from those the wonderful stories of great care.
The reason we pay such a huge sum per capita for public healthcare – £3,600 a year for every man, woman and child in the UK – and get such a totally unacceptable service in return, is that private companies are sucking out the money for profit.
10% of NHS patients are in fact privately treated, overwhelmingly for the cheapest and simplest problems, and private contractors suck 18% of the NHS budget.
I do not pretend that reform is not needed in the NHS – but getting out the private bloodsuckers and removing the profits would be a good first step.
Renationalisation of the NHS is urgently required.
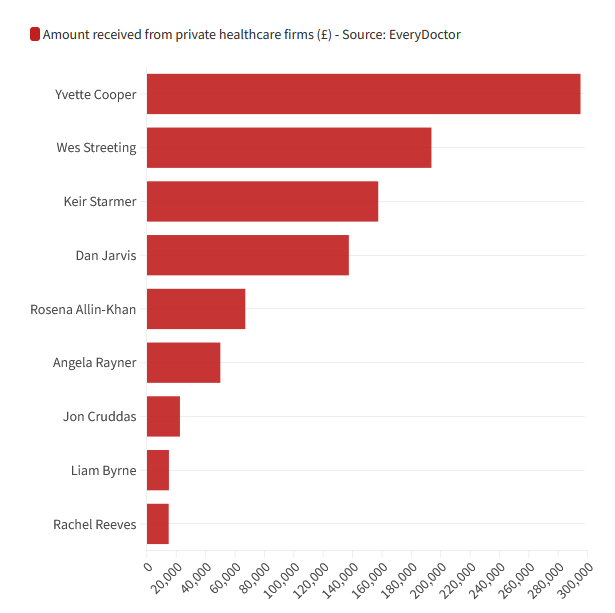
If it were not so profitable then private healthcare lobbyists would not be bribing our politicians. Keir Starmer, Wes Streeting and Yvette Cooper have between them received over £750,000 from private healthcare lobbyists and companies.
As with the Israel lobby, the essential corruption of our politics is what drives the entire policy agenda of the political class. There is an overwhelming case for banning elected politicians and their parties from accepting large donations.
The chances of this happening short of a revolution are zero.
May I urge you to look at this video of the public meeting we held on the NHS during my Blackburn election campaign. Leaving aside my very obvious exhaustion, I was absolutely fascinated by the speeches of Mary Whitby and Dr Bob Gill.
Purely in terms of its content, I think paradoxically this small gathering was one of the best political meetings I have ever witnessed. I absolutely promise you it is worth your time and attention, and you will come out of it looking at the NHS in an entirely different light.
I most certainly did.
————————————————
Forgive me for pointing out that my ability to provide this coverage is entirely dependent on your kind voluntary subscriptions which keep this blog going. This post is free for anybody to reproduce or republish, including in translation. You are still very welcome to read without subscribing.
Unlike our adversaries including the Integrity Initiative, the 77th Brigade, Bellingcat, the Atlantic Council and hundreds of other warmongering propaganda operations, this blog has no source of state, corporate or institutional finance whatsoever. It runs entirely on voluntary subscriptions from its readers – many of whom do not necessarily agree with every article, but welcome the alternative voice, insider information and debate.
Subscriptions to keep this blog going are gratefully received.
Choose subscription amount from dropdown box:
PayPal address for one-off donations: [email protected]
Alternatively by bank transfer or standing order:
Account name
MURRAY CJ
Account number 3 2 1 5 0 9 6 2
Sort code 6 0 – 4 0 – 0 5
IBAN GB98NWBK60400532150962
BIC NWBKGB2L
Bank address Natwest, PO Box 414, 38 Strand, London, WC2H 5JB
Bitcoin: bc1q3sdm60rshynxtvfnkhhqjn83vk3e3nyw78cjx9
Ethereum/ERC-20: 0x764a6054783e86C321Cb8208442477d24834861a
Really good article and video. We are a rich and prosperous country where the politicians of all stripes have spent 40 years destroying the institutions of fairness – the NHS, the Unions, Education, access to the Law, Public Transport, the Benefits System, Care of the elderly and social care etc on the altar of the market. All the while denying the reality of what they are doing.
I agree 166 percent with your comment. The article is point-on and underlines the pathetic downfall of the NHS as we knew it.
Regarding the video, at this point in time, it’s still a bit notional. But sounds promising!
24 years ago.
I could wander into the surgery, without an appointment, take a seat, wait maybe 20 minutes maximum, see my own named GP, have minor procedures carried out, pay nothing (apart from NI).
Today.
Can’t get near the surgery, can’t get an immediate appointment, have to see either a receptionist, practitioner or nurse, if I eventually see a GP they will be a total stranger probably with English not their first language, any procedures will be by referral to the private sector and have to be paid for and there will be no NHS follow up.
What marvellous progress we have made.
In my recent experience, one never sees an actual GP. They have become mythical creatures like the Greek gods – you hear about them and their rules, but you never see them.
I have had minimal contact with the NHS. Apart from occasionally having my ears syringed, back when they did that, being checked for aortic widening by a couple of delightful nurses, and having my eyes examined by a specialist because my optician wasn’t sure (there turned out to be no problem)… oh, and once asking my GP about a swollen ankle and being told “typical reaction to an insect bite”.
In July I noticed some skin discoloration and lumpiness on one of my shins, and decided to “have it looked at”. (Actually my womenfolk insisted). Same rigmarole that others have described, except that as I have no car it involve a mile-and-a-half hike each way – fun in the rain.
Since that first visit I have had four appointments, the first three with different people and not one with an actual doctor. (A doctor did ring me twice, listened patiently, and offered advice). At each appointment I was given a new set of prescriptions; no one has yet given me a diagnosis. Nor was I ever asked to come back or even check in for reassessment to see how the treatment was going; everything seems to be “open-loop”. All four NHS staff who saw me were “nurse practitioners”; three of them told me they were “cheap doctors”.
At my last appointment, several weeks ago, I was asked to take photographs of the affected areas and “send them to us”. This while I was sitting in an examination room a few feet from a nurse practitioner! Nothing could have been simpler than for her to take as many photographs as she saw fit, but apparently that is not the way they do things. I got family members to take photos with a smartphone (another thing I don’t have) and, after a difficult struggle, managed to send them to the surgery. Weeks later I was told that those photos had been sent to the Dermatology Department at the hospital, and the surgery staff are apparently waiting for a reply! The photos, taken by a lay person, are now of course weeks out of date. And presumably, if anyone at Dermatology ever does look at them, I don’t see how they can diagnose much from them. Still, the surgery has got rid of me.
Now I come to think of it, when it comes to the NHS – and most other government services – we are all boiling frogs. The service has disappeared almost completely, but so quietly and gradually that we hardly noticed. If only we had representatives in government who had our interests at heart – but of course we don’t. It’s not as if we lived in a democracy.
166 percent :-))
One of the lowest state pensions in Europe too.
You are quite right about the country’s wealth. Britain is the sixth largest economy in the world. As Joe Guinan and Howard Reed of the Democracy Collaborative point out, Britain’s GDP when the NHS was founded in 1945 was £383bn in today’s terms; it is £2.3tn today. In other words they write, “We are more than five times richer in real terms than Atlee’s Britain.”
https://tribunemag.co.uk/2024/07/no-we-havent-run-out-of-money
That reality is dutifully suppressed by Britain’s opinion formers who generally support the Starmer-Mandelson-Reeves project of endless austerity, privatisation and neoliberalism on steroids.
A fantastic article Craig, as many of your articles are.
I am also old enough to remember the times when the doctor would visit you in the home. It was a fantastic NHS.
I really wish we had people like you in politics.
You would make a fantastic PM.
Wishing you good health.
Z
“We are more than five times richer in real terms than Atlee’s Britain”.
Atlee’s Britain was bankrupt and heavily in debt. The UK government finished paying off its debts to the USA about 20 years ago.
” the politicians of all stripes have spent 40 years destroying the institutions of fairness”
Politicians of all the stripes that are allowed.
In my opinion the phrase ‘Free at the point of use’ is interesting. There will be caveats to how ‘free’ its use is. One may be weight – the others may be Covid jabs etc.
It will only be ‘free’ if you do as you are told.
The main thing Streeting Cooper and all the players at The Gravy Train Station will be pushing is Medical premiums for those who can afford it. There may be an incentive to already well off people to ‘invest’ in their private/NHS healthcare. Say by making it tax-deductible. Because the poor pay very little tax, or none at all, the State Premium will be ‘free’ and the poor will get what they pay for – very little and a longer queue.
Remember Thatcher’s kindness? She went private to get out of the queue so as that poorer people could hutch up a bit. A wonderful gesture.
The big money is in the insurance – more PPI (off balance-sheet spending) paying more for over priced generic drugs – never mind the new expensive drug (which will *be rationed) and more flogging off National Health Assets to Beardy Branson and his mates.
Interestingly when the Oaf Johnson caught Covid he was treated in an NHS Hospital. If the idiot was insured why was he not treated in his Private Hospital?
The answer is easy: Private medical Insurers do not like paying out on long-term illnesses or treatment so he was landed on the NHS.
Heart Attacks – Multiple victims of crashes etc. are not what the Private medical Sector want to cover or pay out on. It’s very costly to them.
So the unthinking idiotic politicians will either after pay astronomic Premiums for full cover or just hope that the Emergency Part of the NHS (its most critical part) is still in existence. Otherwise if Streeting and Cooper are ever in an emergency Ward they will have to rifle through the T’s and C’s to see if they have cover whilst in severe pain.
If they are not covered for emergency treatment and its aftermath (say for life?) then they will be bunged on a ward in the actually failed NHS with a pack of Paracetamol for company and wait in the queues like the poorer ones.
Of course greedy people only think of the money – not the consequences for other – they don’t even think about the consequences for themselves or their families. If they were forward thinking – they would not be MPs.
There are exceptions of course but a lot less exceptions than in the past.
Many Happy Returns Craig. Thanks for being here.
I do hope you still plan to emigrate to somewhere with better health care…
Yes, having helped ruin this country in various ways, let’s hope Craig, at least, has a great rest of his life and sod everyone else who is stuck here.
In the late1960’s whan CM was a child life expectancy was about 71 and now about 81.
Number of elderly people nearly doubled as % of the population.( O/T what would age demographic look like without immigration?)
Quick superficial search indicates that we have more GP’s per 1000 now.
The majority of GPs nowadays DO NOT work five days a week, DO NOT make home visits and DO get paid more than £100,000.
Quantity does not equate to quality.
Oh shit I forgot
All the best CM. Keep fighting
Only for the post war generation; for anybody after the late 1950s, life expectancy has sharply reversed. There is one comfortable generation and the rest haven’t even had secure employment, or a home. That same generation – for reasons outlined – have also not had families, except the more affluent few.
If you are offered treatment in a private hospital on the NHS, reject it.
They can do routine treatment well enough, but if anything goes wrong and you need emergency care, they will dial 999 for an NHS ambulance to eventually take you to an NHS hospital.
Can some knowledgeable person explain to me how the NHS can afford to send patients to private medical providers, who are profit based, but cannot afford to provide that medical care themselves. And, given that a large proportion of private medical staff (Surgeons, consultants) are actually NHS staff is there a conflict of interest or even rampant corruption.
Anecdote
Friend of mine went private for saving time and second opinion. After seeing his own doctor at this private clinic he just turned around and walked away.😀
It can’t. The practice started when DHSC was pushing extremely hard for time targets to be met and NHS was willing to spend a lot of money in order to meet those targets. It has not stopped because there are now fewer doctors and nurses and NHS is desperate to reduce the pressure on the staff that remain.
Wee Jim
Quite.
My point in a previous post entirely.
These greedy Clowns can’t (or won’t) see it.
As I’ve mentioned before. IMO, If you want to improve NHS care you need to ban/outlaw all private care in the country – remove all alternatives – such that everyone has to use the same service.
Most MPs and a lot of senior NHS staff use private healthcare, go figure where their loyalties lie.
Same logic as banning/getting rid of independent schools. When your average level of performance is rotten, improve matters by eliminating the few good performers.
ps. Happy birthday Craig, 66 is really not that old.
The rot continues:
“the Labour Party just oversaw a £1.3 BILLION SELL-OFF of NHS community services to a private equity firm, in Wiltshire.”
https://www.thecanary.co/trending/2024/10/17/nhs-services-wiltshire/
I couldn’t vote for Starmer as it was obvious what his plans for the NHS were – and because of Palestine too.
Many Happy Returns Craig.
I think anybody who reads this blog could write multiple examples of their own – I know I could. I also know a number of GPs who seem to be so well paid that they only need to work a couple of days a week yet still enjoy a comfortable lifestyle. It’s a ‘peas & rice’ mentality that is pretty common in the Caribbean. Can’t knock it. So many anecdotes, no simple solutions.
In my view, most doctors under the age of about 55 no longer behave as professionals – they’re just NHS employees on a certain job grade that carries a fabulous benefits package. They don’t think and just regurgitate ‘guidelines’. I avoid them as much as possible. Whatever your problem might be, they’ll probably suggest there’s a jab for it, as you suggested in your piece above. I don’t trust any of them.
Among the older cohort, a couple of excellent commentators are Drs Carl Heneghan & Tom Jefferson on their substack at:
https://trusttheevidence.substack.com/p/the-nhs-where-does-all-the-money?
Heneghan was probably best known as being a Professor of Evidence Based Medicine at Oxford, as well as a practising medic. In that role he was scathing about the prevailing narrative and insanity throughout the Covid plandemic. He was given the cold shoulder treatment accordingly. The dismissive attitude & rudeness shown to him at the Hallett “No Enquiry” was astonishing.
Evidence based medicine is dead and so is rational decision making throughout government, let alone the NHS. The current series on “Where does all the money go?” is worth a read on the above substack. Then weep.
Ray
The most important thing in my opinion is that the ‘National’ in the NHS needs to be Re-Nationalised.
Actually the NHS is not Nationalised it is a Group of Individual Trusts (Cost Centres).
I’m not against buying in from the Private Sector (I live in France and that’s what they do) but the tail should not wag the dog.
Here (for the moment at least) the French State dictates terms for the Private Sector. How long that will last in France is up for grabs. Unfortunately the French copy the English. Politically/economically they are at the fag end of Blair and heading for Brown.
What a wonderful video thank you very much all concerned. I will share this far and wide. I knew it was true without knowing details.
I can never been able to get treatment for years. It is obvious the GPs are discouraged from making referrals because they have to justify this to higher up the chain. So if you have something novel or difficult to diagnose… as cases could come back on them. So instead of erring on the side of caution, patients are turned away, many distressed, because they are deemed to costly too be healed. Gaslighting is everywhere.
Is there any other “health” system in the world that is based on seeing a “general” medic who gets you put on a “waiting list” for a specialist medic?
That question is like an intelligence test. Many in Britain don’t realise that waiting lists need an explanation.
Why don’t you go on a waiting list when you need your car serviced, for example? The answer is obvious. The people at the service garage know how to keep a diary and allocate time.
The explanation of why the NHS runs on waiting lists is simple. It’s because most specialist medics work in both sectors – private and state. They basically keep two lists. They’ll see you on the state when there’s a gap in their work on the prive.
Also much of the NHS’s crappy offering is based on continued monitoring and monitoring and monitoring for years on end, with tossers pocketing money from the state and just keeping you waiting indefinitely. To take the example of men “of a certain age”, this applies for example to hernia and prostate issues. On the private, you just make an appointment for surgery and that’s that. (I speak from experience, so anyone who wishes to tell me I don’t know what I’m talking about can do one.)
The GP system stinks to high heaven. It’s all based on the idea that the poor smell.
@Craig, it’s not just that they may cut benefits to unemployed working class people who don’t take anti-obesity injections. It’s worse than that and a cull is coming, and this goes back to Malthus, the secret god of the British ruling class, as can be seen in so much of British society. And I say British rather than English, because the Scottish elite are just as poor-haty as the English elite.
“It is not medical treatment. It is not a national health service, it is a notional health service.”
National Heap of Shit would be more like it.
Every day I walk or run past a GP surgery. Five years ago there were people going in and out all the time. I live in a rural area where most people travel by car, and typically there would be 5-10 cars outside. Nowadays it’s a GP’s car and his practice manager’s, if there are any cars at all. They’re probably rubbing themselves off over a grant application.
@Craig – Go on the prive if you have the means, and don’t feel guilty about it. I say this as a man of a similar age to yours. I wish you all the best for your health. Look after yourself, mate. We need you as fit and strong as possible. Put your health first.
A general point: it never ceases to amaze me, how little of a critique in Britain those who see themselves as socialist have of two of the “systems” that really, and really f*cking powerfully, oppress real working class people in their real lives – the “health” system and the “education” system.
Anyone who disagrees, please ask yourself what you think the bourgeois “health” and “education” systems are all about, and answer yourself in 2-3 sentences, and see whether you’re satisified with what you come up with.
Then maybe watch something like “Cathy Come Home” from ~60 years ago.
PS – Who’s the richest person most working class people in Britain will ever meet on a one-to-one basis? It’s a medic, that’s who.
‘Is there any other “health” system in the world that is based on seeing a “general” medic who gets you put on a “waiting list” for a specialist medic?’
Funny you should put it that way, Brian! You remind me of one of my very first jobs, back in 1980. I was hired as a software specialist working at DEC’s remote diagnosis centre in Basingstoke. A big bone of contention with management was the way we were organised to deal with customer calls. (In a way, it was quite similar to an NHS surgery). If a customer had a software problem, the customer would ring up to ask for assistance. The managers hired half a dozen “response specialists” – actually just ordinary, reasonably intelligent and sympathetic lay people with no computer training or experience – to answer calls. They would ask the customers for details of the problem, write them down, and pass the note to a technician like me. The technician then had to call back and actually do something about the problem.
The best thing one could say about this system was that it gave the technician a breathing space to do any necessary “research” such as refreshing one’s memory of the manuals. Otherwise it was a bad idea. The customer had to explain the problem to a non-expert who often got the wrong end of the stick. We techies sometimes smiled at reports of, e.g., “Kobold” compiler issues (where the customer had actually spoken of “Cobol”). Then the customer had to wait an arbitrary period, be ready to take an incoming call, and explain it all over again – this time to a comprehending ear.
We techies kept asking that we should take the calls, but the managers wouldn’t have it. I never found out why. Is it too cynical to suspect that they preferred being in charge of two “groups” of employees rather than just one?
I resigned from the NHS in 1993 because I was sick of the incompetence, negligence and corruption (the usual sort that is endemic in British state institutions). A few years ago, someone I knew needed treatment on an eye and ended up paying an NHS doctor moonlighting at a private hospital. It was distasteful to both of us but given the urgency of the need and the delays of the local NHS and the shite treatment, paying was a way out of her going blind in one eye. Bastards
Keeping taking the money can be the ultimate crime.
Back in the day, I knew about 10 nurses, male and female, who just couldn’t take it any more, who were unwilling to continue talking shit to patients. What there is, has fittted a model of “militarism” for a coupla decades now – the spread in wider society of the values of the army. Where this leads, do we know? Sadly yes, and it’s not a nice place at all, to put it mildly. How do we fight it? Ya gotta think of simple questions, with simple answers.
The problem is, everybody knew Streeting had been bought by big private health investors. It has been there in the parliamentary register of public interests for years. Every MP knew it, every newspaper editor, every political journalist, all the big unions that give money to Labour. They were all very aware, yet none issued the slightest peep of concern, let alone objection, when he was put in charge of the NHS. This isn’t some lone crusade by Wes Streeting. He has the rest of them at his back.
Streeting’s jabs are not so much aimed at providing factory but rather cannon fodder.
Many MANY happy returns Craig! Here’s some music I hope you like (sorry about the ads, but you can skip some of them):
Cara Dillon – After the Morning
https://www.youtube.com/watch?v=qtutdXqleNU&list=PLPynIeKJNhn4hlXjx4roHL40dLyeZ8nXo
Chris de Burgh – Quiet Revolution
https://www.youtube.com/watch?v=WoHKzxnyxo0&list=OLAK5uy_nyPJTNSxSuG-yKZXaM4Ca19jHK-PgFjXU&index=1
Wynonna Judd – Revelations
https://www.youtube.com/watch?v=0_ZLbbQUvVA&list=PLdCdxkzMBUapFOReY8tMOzADTdj2VNTRt&index=1
Nova (Shine Your Light On Me)
https://www.youtube.com/watch?v=R8rIBBqwogI
On a lighter note, enjoy your well-earned state pension! I read so many stories of patients being provided with sub optimal care from the NHS. Granted, I have had my fare share of shit medics/dentists treating me, but more recently whenever there is the possibility of anything serious I have been able to get reasonably quick hospital treatment after a consultation. But, normally it all starts with a phone consultation with a paramedic, pharmacist or nurse. Some of these doctors assistants/associates have been pretty good and none have been terrible. Streeting wants to increase use of private facilities and doctors to improve waiting times but many of these doctors are already working full time. So not sure how it would work in practice.
Private healthcare is nice – a private room, better food – and nobody there after 5.00pm. If you have enjoyed your hip replacement or your cataract op, with doctors and nurses with enough time to talk to you just don’t have a medical emergency later in the day. You will just be waiting for an ambulance like everybody else, everywhere else, and in the queue to be seen in your nearest overcrowded A&E… Planned care only, by all means pay to get it done, but not the full range of medical expertise on hand
No. Outlaw private healthcare. Then all those NHS trained, paid and employed staff in the private sector would be available to the NHS full time to alleviate our suffering rather than increasing their profits.
Would that include people going abroad?
My GF had a slipped disc and all the NHS could offer her was a ‘pain management programme’ – i.e. shed loads of drugs. We found a private hospital and a surgeon, who only does private work, and got it sorted for £8,000. Luckily we had the money; millions don’t, I know, but given the cost of the long term care she’d have needed without it – drugs, physiotherapy, wheelchair, walking aids etc. – it would probably have been more economic for the NHS to have paid for that private op.
The British State is comprehensively structurally dysfunctional, run by mediocre at best people & corrupt as hell.
The simple logic of thinking through consequences, doesn’t meaningfully apply to the regime. In terms of the mundane aspects of day-to-day rule. In any aspect, save maintaining a monopoly of power.
Of course even there things are janky, because of the aforementioned flaws.
… emigrate.
And very few people would choose to train for a medical profession, because your proposal essentially makes medical workers slaves of the State.
“essentially makes medical workers slaves of the State”. No. it would make them civil servants, and btw the current 513,205 civil servants in the UK would not consider themselves slaves, IMO.
No. The numbers of people training in the medical profession is decreasing already, and that’s because of Government and NHS imposed limits. They prefer to steal other countries medical staff rather than invest in our own.
Explain how the ‘ordinary person’ is to afford essential healthcare in a private, profit driven market. The only answer is that they will not be able to, so will die or require state benefits to just survive. Only a callous, well off, bastard would think that that is an acceptable solution.
IMO. The fact is that waiting lists/queues are a politically manufactured fiction. Sure you’ll have to wait for treatment but try to find out how many are on the list and what your position on the list is and you’ll be palmed off with BS.
If the NHS was open, honest and competent, they’re not, they’d be able to publish a daily/weekly updated, suitably anonymised, list which patients could check. This is not rocket science.
Lists/queues meet a political need.
“The reason we pay such a huge sum per capita for public healthcare – £3,600 a year for every man, woman and child in the UK – and get such a totally unacceptable service in return, is that private companies are sucking out the money for profit.”
Unfortunately, the converse is also true: the reason the government funds the NHS to the tune of £3,600 a year for every man, woman and child is so that the private companies can suck out the money for profit without the system totally collapsing. If the private companies went, so would the funding. The service wouldn’t improve.
You’re right that Britain gets less health care for what we pay, than other countries do.
But you’re wrong that the sole reason is that some services are provided by private companies.
In Switzerland, which has excellent health care at a cost just a couple of percent higher than the UK system, all health care is private. Health care insurance is compulsory for all residents (people with very little income get income support) but is intelligently regulated, and there is competition between insurance providers. The cost of the basic level of insurance depends on where you live but not on your medical history.
Use google for details, but to cut a long message short, the key to the Swiss system is intelligent regulation.
Having lived in Switzerland, I agree to a certain extent. However, the fine print shows that there are many issues in Switzerland and not a few are based around who is a ‘resident’ and their status. That aside, all the proposed private healthcare ‘solutions’ for the UK are based on the american model, where ONLY the well off get healthcare.
A proper technical and moral assessment of pros and cons of private healthcare and what we could have, followed maybe by a referendum, has never, and will never, be carried out. Instead we are literally being sold down the river to the highest bidder – AKA, asset stripping.
It’s much more corrosive than you suggest. It depends where you live in the US, whether you are insured, employed and a number of other factors. I suppose that the most important issue is ‘efficiency’. The American healthcare system is a huge bloated parasitic entity of half measures and sticking plaster solutions for deep endemic problems. There is a huge complex multi-layered bureaucratic accounting system associated with the insurance policies, which are so complex that clerical staff must be specifically trained to work in the sector. Detail is overwhelming, as it traces every penny or cent expended on health and and issues accounts with lists of chargeable items and what is covered by a particular policy?
The cost of the US healthcare system is dominated by this infinitesimal bean counting mentality which rewards certain elements of healthcare lavishly and feather beds the insurance company executives administering the system. All that clerical stuff comes at great cost.
The irony is that there is a ‘semi-national’ health service in the form of the Veterans administration with a parallel system of hospitals devoted to veterans and government employees so in many places there is a ‘vet’ hospital in addition to a public hospital and very sparse primary care facilities, i.e duplication. It is egregiously wasteful.
Doctors tend to qualify as ‘specialists’ as there are better rewards for being a specialist. For instance if you have a skin problem you seek out a dermatologist not a GP for initial examination. It is a wonderfully, insanely, inefficient system created to find ways to extract money from patients.
The system in US is now maxxed out and the insurance companies are trying( and succeeding) in undermining the efficiency of the British system by creating the shortages that allow them to promote private healthcare. People like Cooper/Streeting are complicit in this process – I’d say criminally complicit in the destruction of the NHS but they are merely the latest recruits to the process.
The coalition produced shysters like Lansley and Hunt, who dismantled the viability of health services. Nulab grifters like Alan Milburn (small bookshop proprietor) and John Reid were aided by Gordon Brown who mis-financed(PFI) the foray into the private sector to get over the political problems of waiting lists but made the health system unviable due to private finance being handed such favourable terms that it has seriously undermined/virtually destroyed the NHS with debt repayments. I think that Brown deserves special contempt for the unmitigated hypocrisy he played a major part in. A former health secretary is Andy Burnham. I would love to find out his thinking regarding his time as health secretary.
Every Friday I attend a peer-support meeting which invites participants to talk about their lives. Some of the distress voiced comes from identifiable mental health issues (eg depression or anxiety). Some, however arises from power issues: eg “I am worried my landlord will evict me”, or “I am being sexually harassed at work”. People are suffering because of the way our society works rather than because there is something ‘wrong’ with them. Similarly, some people are obese because of the effective marketing of appalling ultra-processed food: the problem is in the food rather than in the person.
Here’s a good article about the NHS etc
https://www.julianrose.info/2024/09/digitally-manipulated-humans-and-medically-assisted-death-set-to-become-the-flagship-policy-of-the-british-national-health-service/
This shit has been going on for at least a decade and a half.
I commend this excellent Ted Talk to the forum:
Privatisation of the NHS: Allyson Pollock at TEDxExeter (29 Apr 2014) – YouTube, 18m 03s
As a baby boomer, some years older than Craig Murray, I feel that I’ve been robbed of ‘my’ NHS.. That robbery is ongoing.
They want to jab folk for everything and if folk don’t comply they’ll be punished within society.. Saw that one taking shape during the Cv19 psyop
Very good Craig, thank you
Brilliant article and video. It seems to me that the best way to fight the system is to set up not-for-profits to compete with the private health companies – what do you think?
You can only compete with the private sector if you have bucket loads of cash you can ‘donate’ to your favourite MP or local government officers. Don’t believe the myth of ‘level playing fields’.
OK I see a source is provided for the money paid to Cooper (Yvette, not Tommy) and S.Treeting but is there any information on how that money is used, and how the payments are made and exactly by whom. Is it a cash payment? Is it tied to some activity or person. Are there anti-laundering measures in place? What limitations on its use exist? Does Yvette (notTommy) Cooper just hand over to hubby Ed and say ‘go off to the races for a day and have a Ball’? One must assume that someone like Yvette will pass it on to the favourite think tank/charity/employ an extra spad to research specific health matters, e.g What are the primary health care measures in rural Illinois for uninsured, divorced women? The devil is always in the detail.
Thanks for the article. I was disillusioned with the NHS by about 2015. I was in total disagreement with the GP about statins, blood thinners and blood pressure drugs. I think I won; he admitted I knew more than he did on key topics. I also noted that the tests they offered me were always the ones for which they got handsomely paid, not the tests that most determine a person’s long-term health. I had to request those.
The NHS has always been too centralised. Most of it should have continued the work of the pioneering ‘Peckham Experiment’ 1926-50. Instead we have endless drug-pushers, sorry ‘medics.’ whose training is largely funded by pharma and who can’t think independently. Many competent and ethically-minded medics. left the NHS or were ‘struck off’ after ‘COVID’ because they were unwilling to abandon their professional status and become technicians who just obey orders from on high. That’s how bad it is.
I too ‘left the NHS’ by de-registering from any GP. At 70 I’ll take my chances. Eat good food (many Greeks do; most Brits. prefer it ‘ultra-processed’), exercise and avoid major stress. Oh, and ignore NHS advice on saturated fat and salt if not more.