Latest News › Forums › Discussion Forum › SARS cov2 and Covid 19
- This topic has 1,202 replies, 1 voice, and was last updated 4 years, 3 months ago by
Dave.
-
AuthorPosts
-
May 13, 2020 at 19:25 #53387
Clark
SA, how much is known so far about covid-19 causing neurological damage?
May 13, 2020 at 19:30 #53388The ICL model hasn’t updated for days. Daily infections and daily deaths are stuck on May 7, and Rt is stuck on April 30.
Surely the government’s policy must leave it open to legal action?
May 14, 2020 at 16:24 #53421SA
Clark
Sorry not coming back to you about neurological involvement in Covid-19. There are a couple of papers mainly reviewing findings but no definitive studies. There is evidence that some patients experience loss of smell and taste at the beginning of infections. There is also some evidence of encephalopathy and such like that occur in patients who are very sick. Most of what I can see is non-specific and probably transient, but there is nothing definitive yet.May 14, 2020 at 17:58 #53424SA, covid-19 and neurological effects – link.
May 14, 2020 at 20:09 #53430Yes Clark. This is a review not a systematic study. Yes cases have been described with two mechanisms, an encephalitis or encapholopathy and immune activation. Not very definitive and no hard data. Of course further study will show whether this is something to worry about and specific to covid-19
May 15, 2020 at 12:45 #53461michael norton
Interesting that our last prime minister was diabetic one
and the new prime minister is obese, though it has not been said he is diabetic two.
Boris was seventeen and a half stone when he caught covid-19.
Boris is now determined that we all reduce our weight.May 15, 2020 at 13:28 #53473N_
A nurse in the US blows the whistle on how patients “with Covid-19” are being murdered.
Meanwhile in the holy NHS in Britain all non-urgent surgery has been cancelled, and many wards in many hospitals are empty, while GPs send out “Please sign ‘Do Not Resuscitate’ forms” letters to patients suffering from chronic illnesses.
From what @Clark says, it seems that ambulance workers are being given a lot of makework, scrubbing their vehicles for hours on end. It is unclear whether more person-hours are being worked by nurses than before, but surely the answer is no, given that Intensive Care Unit use has risen but not hugely, whereas much of the other stuff has mostly shut. Using nurses who haven’t had much training to work ventilators may be connected with how the use of ventilators is killing people, as described in the above video.
And you ain’t seen nothing yet.
Reminder: reported Covid-19 deaths divided by reported Covid-19 cases (what is known as the “case fatality rate” is SIXTEEN times higher in Britain than in Russia.
May 15, 2020 at 13:32 #53474PPE is what media consumers and also nurses are being “nudged” to think is a crucial issue. Similar propaganda is run in the army. In the general population for a while it was toilet paper. How the Behavioural Insights Team must laugh. I seriously wonder how much critics know about propaganda sometimes,
Meanwhile, the harvest won’t come in. That’s a bit of a bigger issue than a flu-type bug going round.
May 15, 2020 at 15:35 #53483Covid-19 is a SARS-like illness, not a flu-like illness. Covid-19 is caused by a virus called SARS-CoV-2, a relative of SARS-CoV which causes SARS. Covid-19 has an infection fatality rate of between 1% and 1.5%, over an order of magnitude higher than seasonal flu.
PPE is a crucial issue because covid-19 disproportionally kills medical staff. In the UK, 10% of staff are absent due to covid-19. Covid-19 has been killing medical staff since it first emerged in Wuhan. It killed the young doctor, Dr. Li Wen-Liang, who defied Chinese authorities to alert the world to this new disease. Try watching this:
Coronavirus: How the deadly epidemic sparked a global emergency – 46 minutes, with citizen phone video from within the Wuhan lockdown, including a visit to an overwhelmed hospital, where staff were in despair:
If you have any genuine interest in the use of ventilators, the latter part of this article is informative:
The Great Ventilator Fiasco of COVID-19 (MedPage Today)
I suspect that what has happened is that the UK NHS prepared for ten times as many cases due to the UK government’s initial policy of mitigation, before it was persuaded to implement the more suppressive policy of the stay-at-home restriction and closing pubs and other non-essential businesses.
It is misleading to consider Intensive Care Unit capacity and occupancy in isolation because serious (as opposed to critical) cases are accommodated in “general acute beds” rather than intensive care. There are currently 1,559 critical cases in the UK. The following article is from April 13; pressure on hospitals has eased since then, partly because so many patients have died. Link to article:
* – Figures from the national NHS operational dashboard, seen by HSJ, show that 40.9 per cent of NHS general acute beds were unoccupied as of the weekend — 37,500 of the total 91,600 relevant beds recorded in the data. That is 4,500 more than the 33,000 the NHS said had been freed up on 27 March, and nearly four times the normal amount of free acute beds at this time of year.
* – Despite hospitals remaining relatively empty overall, according to the dashboard data, certain services and settings, especially in some regions, are under high pressure, and maintaining service levels is becoming more difficult with high levels of coronavirus-related staff absence.
* – The dashboard confirms hospital pressure is concentrated on critical care. Across England, 3,228 patients were in critical care beds — representing 78 per cent of the total of 4,122 critical care beds which were available in February. More have since been opened, but it is not known how many.
* – On top of this, thousands of covid-19 patients are receiving basic oxygen support but are not on full critical care ventilation. The dashboard data show this number to be more than 8,100 nationally, or about half of the coronavirus cases currently in hospital.
RUSSIA
Moscow went under lockdown on March 29, at which time there had been only eight deaths in Russia. By comparison, the negligent UK government waited for 359 deaths before locking down. In Russia, much stronger restrictions than the UK’s had been applied progressively throughout March. The earlier restrictions are applied, the less deaths follow; see my table in the latter part of this comment.
– – – – – – – – – – – – – – –N_, it took you moments to reinforce the right-wing distortions and disinformation. It has taken me over an hour to gather evidence to counter your damaging contribution. Please tell me, what is your attitude toward human suffering?
May 15, 2020 at 18:41 #53582“<i>CTs are rife and deter from proper discussions.</i>”
No, but people who say things like that do. They want any kind of criticism of the medical, scientific or other “professional” priesthoods (and of the elite that they all serve) that actually GOES SOMEWHERE to be thrown out alongside stories about Elvis Presley living on the Moon. Anti-conspiracism is mostly not honest, but when it is honest it demeans the person who is coming out with it. It makes them not worth discussing with.
May 15, 2020 at 19:09 #53585“Meanwhile, the harvest won’t come in. That’s a bit of a bigger issue than a flu-type bug going round.”
The harvest may or may not come in whether there was a lockdown or not. Just think ir through, Sick men cannot bring the harvest in.
But as long as you follow the original Trumpian line that it is only the flu, and as long as you also follow the capitalist’s line, that the harvest can be brought in by the workers, who are disposable then a very good Marxists you will prove not to be.May 15, 2020 at 19:35 #53588The naming stuff is marketing. It’s the same as for airports.
SARS-CoV2 [1] is a virus of the same type as the viruses that cause the common cold (namely it is a coronavirus [2], a subtype of that type being SARS), but the symptoms (if a person gets any symptoms at all) are often more severe than for the common cold (as they are for influenza [3], another group of viruses that cause respiratory symptoms that can be severe and can be fatal); and many SARS-CoV2 infectees especially if they are elderly and already have a chronic illness – such as a long-term respiratory illness – are at risk if hospitalised of catching pneumonia (in hospital) and then snuffing it, and indeed they are at risk of snuffing it even if they don’t catch pneumonia in hospital, or if they don’t go to hospital – all of which also apply to flu. So all in all it seems quite flu-typy even if the mortality rate is higher.
Meanwhile the Coronavirus Act means that no hospital looks like it will be successfully sued for causing the death of a Covid-19 certificated patient by improper use of a ventilator and in any case the requirements for cremation paperwork have been relaxed. So of course we’ve all got to clap “the NHS” and “nurses” which really means the medical priesthood, the government, and the state. (Nurses who blow the whistle aren’t getting much of a hearing.) Never underestimate the hypocrisy of the ruling class.
Most scientists don’t have a clue what’s going on, and those that do have a bit of a clue won’t be talking in public. Those who think they know what’s going on will be kept away from the very centre by dint of being village idiots. (It’s very easy for a person who plays a Knower role to an appreciative workplace audience or to some other lower-status audience to get the idea that they know stuff that they don’t. This is the reason why some independently-minded aristocrats even if impoverished prefer to socialise with independently-minded proletarians than with managerial or professional types.) The first big question is this: what amount of biological warfare [4] is there in various aspects of this epidemic? [5]. There is no reason to believe that those who are concerned with national strategy at the helm of the state are able to answer that question with much precision. That said, the answer is obviously not zero.
Notes
1) Is “SARS-CoV2” WHO-decided, i.e. a Big Pharma-decided, name?
2) My guess is that most people don’t know that the scientific priesthood uses the word “coronavirus” for the viruses that cause the common cold as well as for SARS, and that having had their minds softened up by the media many would think that anybody who told them this fact was probably a nutter.
3) Many believe that when they have a fairly heavy cold that disappears within a day or two, or maybe three, that they actually have “flu”, when usually they haven’t, because flu usually knocks a person out for longer and with a bigger hammer.
4) A pandemic is a type of epidemic, so I am using the word “epidemic” correctly even if many have been encouraged to use a word that is new for them, namely “pandemic”. Getting people to use a word that is new for them is a known propaganda technique that encourages them to think they are in a “community” that is “with the programme”.
5) This is why I keep on about the disparity between Britain and Russia for case fatality ratios. Obviously testing policy, type of test, the criteria for deciding whether or not to slap a Covid-19 diagnosis on a patient who is in this or that health or demographic category, and policies regarding sanitising hospitals all have an effect on the CFR (as doubtless does climate), but I suggest that when Britain has a CFR that is 16 times higher than Russia’s there are almost certainly other major human-caused factors.May 16, 2020 at 12:06 #53611N_
Your post contains a lot of incomplete information an some that are completely wrong
SARS-CoV2 [1] is a virus of the same type as the viruses that cause the common cold (namely it is a coronavirus [2], a subtype of that type being SARS), but the symptoms (if a person gets any symptoms at all) are often more severe than for the common cold (as they are for influenza [3], another group of viruses that cause respiratory symptoms that can be severe and can be fatal); and many SARS-CoV2 infectees especially if they are elderly and already have a chronic illness – such as a long-term respiratory illness – are at risk if hospitalised of catching pneumonia (in hospital) and then snuffing it, and indeed they are at risk of snuffing it even if they don’t catch pneumonia in hospital, or if they don’t go to hospital – all of which also apply to flu. So all in all it seems quite flu-typy even if the mortality rate is higher.
Yes SARS-Cov2 is the same family as some common cold viruses but this is the way that scientific classifications operate. So for example strawberries, apples and roses all belong to the same natural botanic family the Rosaceae but they are completely different in many ways. So belonging to the same family does not make it less severe or more severe, this is an inherent quality of the organism. Secondly the symptoms, if present, are sufficiently different from those of influenza. They are a high temperature, a dry cough, shortness of breath, and less commonly sneezing and stuffy nose, although these may also occur. Also whereas in influenza you may get a secondary bacterial pneumonia, in Covid-19 the major serious pathology is a picture called Acute Respiratory distress syndrome, where the lung air sacs fill of inflammatory fluid and there is no secondary bacterial infection. This is crucial because antibiotics may help some who develop secondary bacterial pneumonia in influenza, but have no use in the management of covid-19. So it is not flu like in any shape or form and persisting to use this expression denotes wilful distortion. This I=has been stated time and time again and you should know.
Meanwhile the Coronavirus Act means that no hospital looks like it will be successfully sued for causing the death of a Covid-19 certificated patient by improper use of a ventilator and in any case the requirements for cremation paperwork have been relaxed. So of course we’ve all got to clap “the NHS” and “nurses” which really means the medical priesthood, the government, and the state. (Nurses who blow the whistle aren’t getting much of a hearing.) Never underestimate the hypocrisy of the ruling class.
What exactly do you mean by the improper use of a ventilator? I do not think that there is a blanket waiver on medical negligence because of covid-19 if you look at the law carefully. What exactly do you mean by the “medical priesthood”. Is that a known CT term? Is there a pope and priests and so on? Is medicine a religion? This is a wilful distortion to imply that a profession is conspiring for its own sake, against the public and is baseless.
Most scientists don’t have a clue what’s going on, and those that do have a bit of a clue won’t be talking in public. Those who think they know what’s going on will be kept away from the very centre by dint of being village idiots. (It’s very easy for a person who plays a Knower role to an appreciative workplace audience or to some other lower-status audience to get the idea that they know stuff that they don’t. This is the reason why some independently-minded aristocrats even if impoverished prefer to socialise with independently-minded proletarians than with managerial or professional types.) The first big question is this: what amount of biological warfare [4] is there in various aspects of this epidemic? [5]. There is no reason to believe that those who are concerned with national strategy at the helm of the state are able to answer that question with much precision. That said, the answer is obviously not zero.
Thanks N_ for that information. I take it that unlike most scientists you are fully conversant with what is going on. You have done your research by visiting sites on the internet and found the truth? The rest of the passage above doesn’t make much sense.
And so on you go especially with your self-important notes not based on facts. Why do you do this?
May 16, 2020 at 12:42 #53614SA,
N is doing it because he is using free will, he has a brain and as of now, it is not yet against the law to question.
Our U.K. government seem to not want us comparing one nearby country of similar population numbers with the U.K.
they say things like, there is no usefulness in comparing how one country deals with covid-19 with another country.If one were allowed to express an opinion, one might imagine the U.K. authorities have much to hide.
It is almost certain, (in my view) that bat hunters have been in bat caves in South West China, for the express purpose of identifying viruses.
What they do with a “new” virus, we do not know.
However, to imagine there is no Chinese government involvement with these viruses is absurd.May 16, 2020 at 13:04 #53621N_, May 15, 18:41, #53582
– “They…” [those who use the term “conspiracy theory”] “want any kind of criticism of the medical, scientific or other “professional” priesthoods (and of the elite that they all serve) that actually GOES SOMEWHERE to be thrown out alongside stories about Elvis Presley living on the Moon. Anti-conspiracism is mostly not honest, but when it is honest it demeans the person who is coming out with it. It makes them not worth discussing with”
The terms “conspiracy theory”, “conspiracy theories” and “conspiracy theorist” are clearly a problem. I regard conspiracy theory (in the general sense, as in gravitational theory, Marxian theory, theory of music etc.) to be characterised by “argument primarily from motive”. N_, would you read this please?
Then, we should consider and achieve consensus on one point at a time, to keep things focussed.
May 16, 2020 at 13:08 #53623Michael
Off course the British government (or should I say the regional English government) is either really at sea with this crisis or are up to something which they are not telling us. The wilful confusion created by each announcement is staggering. Take this latest announcement from Hancock about R, the rate of reproduction of the virus. It seems that the government is now saying that the R value of 1 is OK, but in fact I do not think they know, or will admit to know what the real value is. Suddenly we are being told that the R value ‘overall’ in London is 0,4 but that the value is higher overall because of high rates in care homes and in hospitals, as if those do not matter.
Coronavirus: Suddenly, the government isn’t so sure the R rate is importantTake the words of the prime minister. On 30 April, Boris Johnson told the nation that “keeping the R rate down is absolutely vital to our recovery”.
Or take the words of Monday’s government document, “Our Plan to Rebuild”, which made a point of warning that the R rate was “potentially only just below 1”.
On this basis, the document suggested, the government was only allowing the smallest of lockdown easing to take place in England.On the advice of the government’s scientific advisory committee SAGE, the government announced on Friday evening that the R rate had gone up.
The range, now from 0.7 to 1, means there is now a chance that the rate of infection has stopped declining in the community.
Suddenly, it feels if the government isn’t quite so sure of the central role of the R rate.
Government scientific advisers stress the R is rising because of the scale of infections in care homes and hospitals, not because it’s going up elsewhere in the community more generally.So now, comparison with other countries is not useful, and also the R value doesn’t mean anything. But in fact the weekend announcement has actually led to many thinking that the lockdown is now lifted. Shops are reopening and some with no obvious attempts at social distancing from my personal experience on a quick drive yesterday. The traffic is coming back and the tube trains, according to the news outlets, are now crowded again.
And meanwhile “Coronavirus: Estimated speed of coronavirus infections rises over past week ”
And this is before the last easing of lockdown.
I am not against attacking the government but I am just pointing out that N_ is indulfing in futile arguments about facts that have long been settled. His persistence in calling this ‘flu’ has no basis and if he concentrates on attacking the government rather than the profession then he is barking up the wrong tree and in fact helping the government’s incompetence and its coverup. Similarly I think going on about Chines culpability is a useful tool for our governments blatant incompetence.-
This reply was modified 4 years, 2 months ago by
modbot.
May 16, 2020 at 13:21 #53624– “N is doing it because he is using free will, he has a brain and as of now, it is not yet against the law to question.”
Indeed. But if they can get you asking the wrong questions, they don’t have to worry about the answers, do they?
Michael, they’ve effectively diverted your attention from the US/UK governments onto the Chinese government. N_ is right; there has been much lower mortality per population in Russia than in the US/UK. That difference will remain, no matter what the Chinese government did. It’s bad in the US and UK because our governments fucked up. The Chinese government also fucked up, fucking horribly, but that’s for the people of China to address, just as it’s for the people of the US/UK to address our governments. We the people don’t have aircraft carriers and ICBMs (thank the Goddess); we can’t project our power thousands of miles. All we have is ourselves.
May 16, 2020 at 13:32 #53627Indications are emerging that all the shit-slinging between the US government and the Chinese government is that it was a joint research project that fucked up. The US very quickly and quietly withdrew funding from it at the same time as the US intel agencies briefed that the virus was probably a lab escape.
Of course, neither government want attention paid to that, so they’re indulging in a shit fight to distract their own populations.
May 16, 2020 at 14:04 #53628Good news that our Prime Minister is FATY.
That he has been taken to the brink of intubation, not quite but almost.
He was seventeen and a half stone.
He is now on the road to understanding that bluff and bluster do not work against covid-19.
He is a committed cyclist and wants to make cycling to work, if possible the norm.
Good.
Now we need some truth, does diabetes cause you to get FAT or do fat people become diabetic.
Part of the reason people who are diabetic have done so badly after they have contracted covid-19 is visceral fat, which already causes damage to their organs.May 16, 2020 at 18:45 #53643Michael
Being obese (the clinical term used for fat-and there are grades-overweight, obese, and grossly obese) makes you more susceptible to diabetes, hypertension and heart disease, referred to as ‘the metabolic syndrome. It makes you more susceptible to heart disease and stroke. 29% of adults are classified as being obese, that is almost one in three people. Losing weight reverses these risk factors. So if our PM wants to set an example he should lose weight to something between 11 and 12 stones.May 16, 2020 at 19:02 #53644SA
quite, one of my friends was nineteen stone and discovered he was type 2, he has lost eight stone, over about four years, essentially he has reversed his diabetes but his GP surgery still classes him as diabetic.
My friend does not eat for one hundred hours, in a go, each month.
He does not eat for eighteen hours each day, taking his two meals in the six hour window,
he is now quite fit. He does not ( or tries not to) eat sugar, bread, cakes or sweets or carbonated drinks, nor does he eat tv meals nor does he eat take always, all these things he used to indulge, he still modestly drinks alcohol.
His gp surgery told him the exact opposite of what he did.
Diabetes is one of the worst things to attain, yet so many of our people are now Type Two.
Let us hope Boris pushes his ideas, to cut sugar based foods and get us outside and walking, running, canoeing and swimming and cycling.
Part of the reason we seem to have such a lot of covid-19 deaths in the U.K. is because of diabetes, overweight and unfit, most people, even young people are very unfit, I would say they are bringing themselves towards an early death by their own mouths.
This is the time for a health revolution.May 16, 2020 at 21:35 #53651The creation of the “Are they lifting the lockdown too fast?” channel for public opinion in Britain suggests that the ruling elite will soon try to enforce compulsory testing on all school pupils in that benighted country.
What a big propaganda push there is, complete with media articles talking about “100% accuracy” in testing! WTF kind of test is that then? It must be the first 100% accurate (100% true-positive, 100% true-negative) test in medical history! How clever the “scientists” must be to
have been paid by Big Pharma tosay they have come up with it so quickly!Compulsory vaccination will probably follow, quite possibly with smartphone “contact tracing” mixed in with it. It wouldn’t surprise me if they claim, even if only to Daily Express readers, that the vaccine is 100% successful too. Wow – another first in medical history.
Never mind that annual “flu jabs” have probably contributed a lot to weakening people’s immunity to viruses. They can’t be much good if their stimulation of your antibody mechanism only lasts a year, can they? People are literally being treated the way pet vets – working in a profession dominated by US multinational Colgate-Palmolive which owns Hill’s – treat pets.
How stupid a person has to be to get annual flu jabs! Try zinc. Try bee pollen. Try nigella seeds. All three are accepted even by “ekshpurtz” to strengthen the immune system. How many slavish getters of annual flu jabs could even give a damn about that?
How about somebody plots annual flu jab consumption against Covid-19 mortality rate for different countries? I’m guessing that a significantly greater proportion of the population gets annual flu jabs in Britain than in Russia.
In Britain people look up to medics like nobody’s business, which causes the warped mind and persona of a medic – a career phony if ever there was one – to treat them with even more contempt.
In Russia, most medics are much lower-paid and you could even argue that many of them are actually proletarians or maybe lower middle class. At least most of them don’t live in mansions at the top of the hill and take six or more holidays a year to “resorts” that cater for people with more money than sense, as many British medics do.
Both compulsory testing and compulsory vaccination must be resisted.
To detourn Bertolt Brecht:
“Mass vaccination resistance: the stupid call it stupid and the squalid call it squalid.”
May 16, 2020 at 23:54 #53656– “What a big propaganda push there is, complete with media articles…”
You must consume a lot more “news” media than me.
– “I’m guessing that a significantly greater proportion of the population gets annual flu jabs in Britain than in Russia”
Possibly, or maybe it makes no difference, or maybe flu jabs even help. That’s what cohort studies and case-control studies are for.
But consider the first order effects first, and in the case of an infection that multiplies as fast as covid-19, that’s timing. Russia’s lower mortality totals are the result of their stronger and especially earlier social restrictions. 8 deaths at time of lockdown in Russia, versus 359 in the UK, and Russia started taking precautions in February.
– “Both compulsory testing and compulsory vaccination must be resisted.”
There’s nothing quite as thrilling as counting your vultures before they’ve hatched.
May 17, 2020 at 09:40 #53668Well, I wanted to ask why is the number of reported covid-19 deaths 1/13 of those counted in the U.K.
Similar number of covid-19 victims counted ( now slightly more in Russia),
this seems an improbable difference?May 17, 2020 at 12:10 #53689– “now slightly more in Russia”
It’ll keep going up.
Timing is the most important matter to get our heads around; many of the mistakes are because people look at a static snapshot, but covid-19 doesn’t stand still. The infection rate increases if it can, when social restrictions are light enough, but we never know how many are infected, because 80% of the infected have no symptoms, and 100% of the infected are infectious before symptoms show.
The best estimate we get comes two weeks later, as the deaths show up. Then we can estimate how many must have been infected two weeks previously. That’s how the (unfairly maligned) ICL model works.
In Russia, a higher proportion of cases are getting detected because Russia does more tests per head of population. Russia is also a big place, so there is less travel between far-flung cities, less dispersion of infection, relatively speaking, so the authorities have more idea where to target tests.
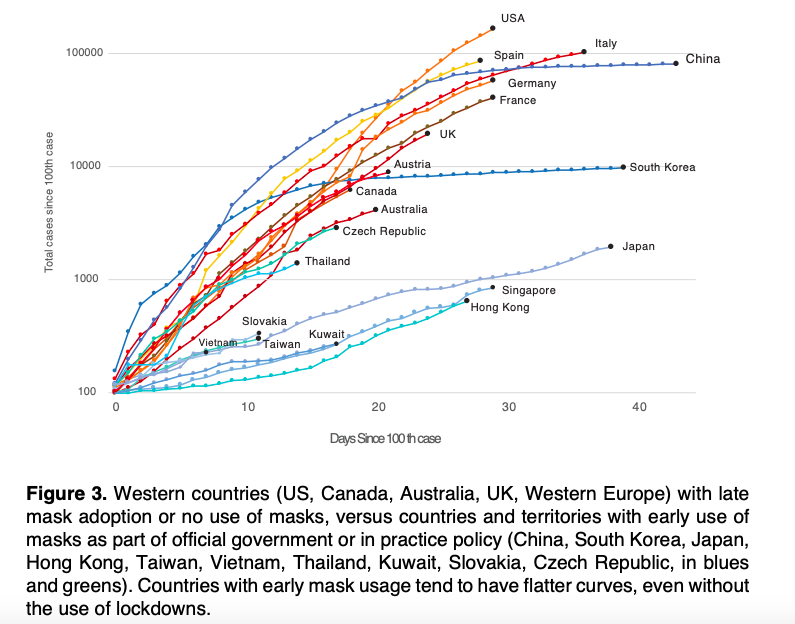
Comparing how well or badly countries are doing is best revealed by plotting on one graph deaths against time for each country. That gives a load of curves rising at different rates. But the crucial step is to shuffle each country’s line horizontally, to align all their starting points to a fixed number of deaths, to remove the differences created by the pandemic arriving at different times in different countries.
Here is one such graph, for comparing countries mandating face masks against countries that don’t. The graph is from about 40% down in this systematic review. Unfortunately the starting points were aligned by cases rather than deaths, and the comparison is thus subject to distortion by how much testing was done and how testing was targeted – ironically, better testing makes the country’s problem look worse. The graph also doesn’t include Russia, but it does show you the type of graph you need to find.
Note that the vertical axis in that graph is logarithmic; each higher horizontal division is a factor of ten greater. The straightest lines would be curving upwards if the “number of cases” axis was linear; such “log-linear” graphs turn exponential growth into a straight slope. Note lines that curve towards the horizontal; that indicates the effect of social restrictions.
-
This reply was modified 4 years, 2 months ago by
-
AuthorPosts
{kind=link}
- The topic ‘SARS cov2 and Covid 19’ is closed to new replies.